
Oxford tackles Bundibugyo, detecting Cyclospora, & 500k comments points to "no"
No. 19 | July 16, 2026

Let’s get into this week’s cup of biotech tea. ☕ If you only have time for one this week, I’d start with #3!
Taking an important step toward better preparedness for Bundibugyo ➡️
The oral psoriasis competition continues to heighten - a new antagonist ➡️
How do we detect the parasite, Cyclospora, that has the U.S. in a panic? ➡️
Overwhelming public opposition to the proposed OMB grant funding changes ➡️
Exploring Cyclospora misinformation & why poor surveillance made it worse ➡️
Bonus (paid): Laboratory-Developed Test ➡️
1. Story I’m Watching
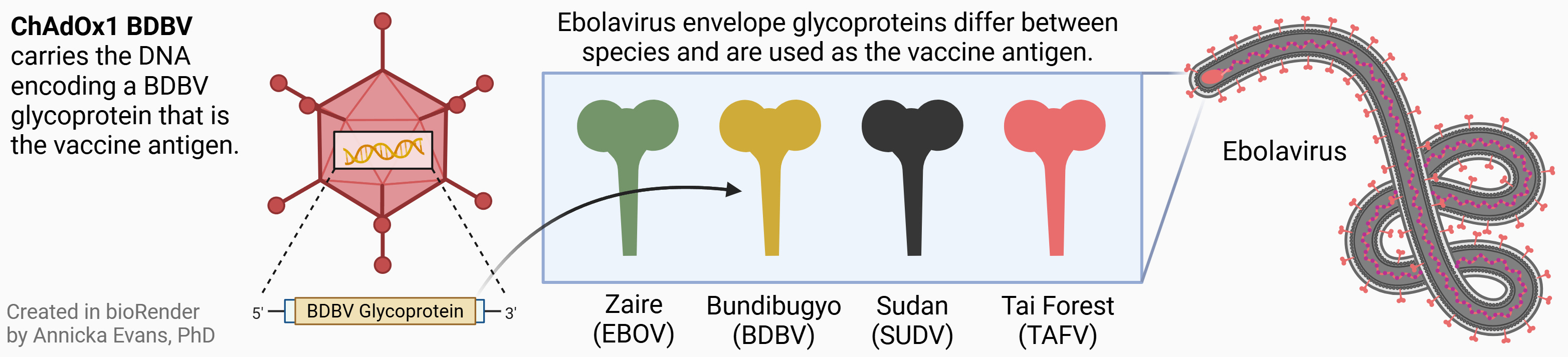
The Tea: While the headlines have slowed, the Ebola outbreak in DR Congo has unfortunately continued. I was really thrilled to see that The University of Oxford has begun clinical trials of the ChAdOx1 BDBV (Bundibugyo ebolavirus) vaccine. Despite this not being the first Bundibugyo outbreak (initial outbreak was 2007), we’ve (globally) failed to invest the time and money to get a working vaccine across the finish line. So even just initiating clinical trials is a moment to celebrate.
Recruitment for the trial has begun, which will assess safety and how effectively the vaccine triggers an immune response. They are aiming for 50 healthy adults.
A few more sips: ChAdOx1 BDBV, developed by Oxford’s Vaccine Group and Pandemic Sciences Institute, carries DNA expressing the BDBV glycoprotein inside a weakened adenovirus shell.
2. From the Bench
The Tea: A few weeks back we covered a new oral psoriasis med, as an alternative to the landscape of injectables, with promising data. We discussed how the IL-23 landscape is moving toward this more convenient route of administration.

This week we’re looking at another new oral drug for psoriasis. It is being developed by Avere Therapeutics, which just went public earlier this week! AVR-001 is an interleukin-23 (IL-23) receptor antagonist, blocking the binding of IL-23 to it’s cytokine receptor. I took the previous figure and updated it to include AVR-001 and denote which of the meds of each mechanism of action are oral versus injection.
As you can see, AVR-001 has a competitor — Icotyde (made by J&J) — which was approved earlier this year. What’s different? Mostly the dosing schedule. While Icotyde is a once-daily medication, AVR-001 is being developed as a once-weekly. Finally, you can see that the injectable space is saturated with options. The newer drugs are investigating other mechanisms of action that can be as safe & effective while allowing for formulation in a pill.
Message me if you have a recent science development you’d like to see featured!
3. Bio[Tech]
The Tea: If you hadn’t heard of the parasite known as Cyclospora before this month, you most likely have now. As the United States experiences unusually high numbers of cyclosporiasis (as of writing this, the current outbreak has sickened almost 7,000 people in 34 states), I wanted to dive a bit into the diagnostic tests used to detect it.
Molecular-based gastrointestinal (GI) screening tests are very sensitive and have the ability to detect multiple targets at once. Hospitals that receive patient stool samples either send them out to a certified lab for the test to be run, or run them in-house if they’ve adopted the technology. There are a handful of approved PCR tests that detect the presence of select bacteria, viruses, or parasites that could be the culprit when a patient comes in with GI symptoms. In particular, these include Cyclospora:
BioFire GI Panel Mid (developed by bioMerieux)
EasyScreen GI Parasite Detection Kit (developed by Genetic Signatures)
QIAstat-Dx (developed by Qiagen)
Gastrointestinal Pathogen Panel (Mayo Clinic LDT)
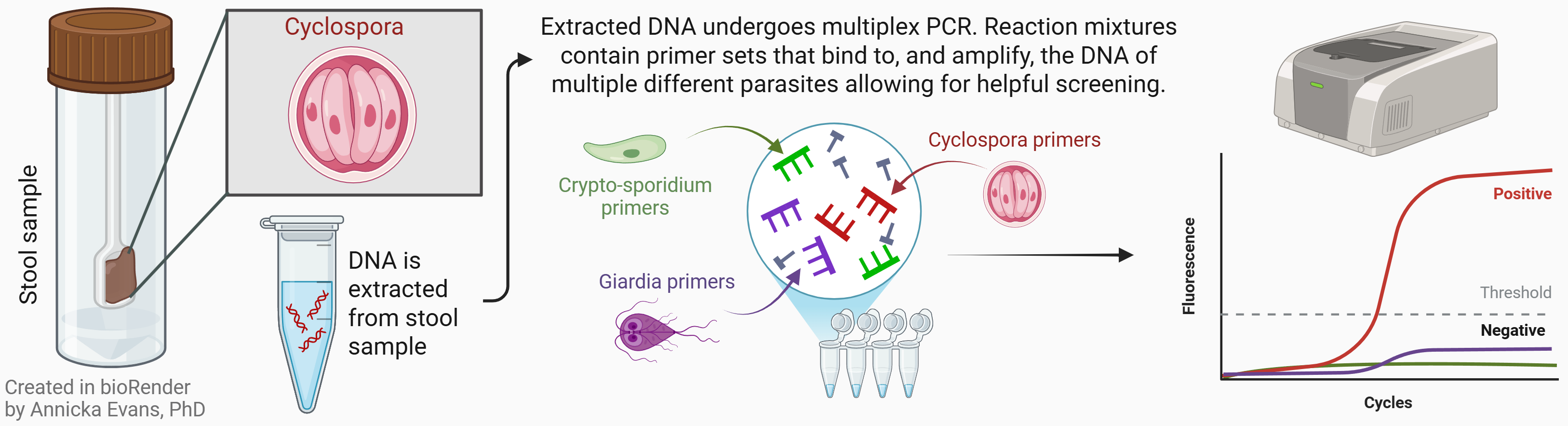
A few more sips: Some labs or hospitals may not be set-up for PCR testing and opt for more standard microscopy techniques. The problem is that the amount of shed parasite in the sample is often really low resulting in poor detection. It’s recommended consecutive stool samples from multiple days are tested to confirm a negative result. Hospitals should seek out molecular-based testing!
4. The Rulebook
The Tea: A few weeks ago we covered the OMB proposed changes to grant funding (2 CFR part 200) with public comments closing just this week.

The count of responses alone (nearly half a million!!!) demonstrate how serious people feel about the implications of the changes.
An early analysis out of NC Chapel Hill (using AI classification that, of course, will only give us a preliminary view of outlook) showed that about 95% of comments were in opposition of the changes - an overwhelming majority. While it only captured the first ~50k responses, if the subset is a representation of the whole, a revisit of the proposed changes is warranted.
5. The Human Side
The Tea: In this opinion piece, Katrine Wallace, PhD talks us through both why the U.S. has been unable to identify the source of the current Cyclospora outbreak & the dangers of the misinformation that has been circling.
And while Cyclospora, is difficult to trace at baseline, the underlying cuts to surveillance and staffing last year, have undoubtedly made this worse. In the wake of a prolonged period of no identified source, Dr. Kat discusses the danger of the “invented certainty” that circled the internet while the public searched for ways to reduce risk.
“False reassurance is not a neutral outcome. It is a risk that looks like safety.” - Dr. Kat

Biotech Term of the Week
Paid Subscriber Bonus Content
Laboratory-Developed Test
