
Standing ovation data, editing heart risk, & a tighter grant leash
No. 13 | June 4, 2026

🎉 Lucky Issue 13!!!
I’m thrilled to see this community grow faster than I imagined. To celebrate, I’m opening 10 early supporter spots at 33% off for life ($20/year) ☕
Paid subscribers get the Biotech Term of the Week, where we break down biotech concepts, technologies, or terms you’ll encounter again & again in the industry. We’re starting a new series, and I’d love more readers to join us.
Let’s get into this week’s cup of biotech tea. ☕ If you only have time for one this week, I’d start with #1!
Researchers get a standing ovation for pancreatic cancer data ➡️
A gene editor for cholesterol reduction may change heart disease treatment➡️
Sleep apnea detection using Apple watch sensors➡️
Proposed change to grant review tighten criteria & shift priorities➡️
The story of an American ER physician surviving Ebola➡️
Bonus (paid): Grant Programs (1st of FDA Encouraging Innovation series)➡️
1. Story I’m Watching
The Tea: It’s likely you’ve heard (or seen videos) about the standing ovation earned by Phase III clinical trial results for pancreatic cancer drug, daraxonrasib, presented at the American Society of Clinical Oncology (ASCO) annual conference.
The trial showed that daraxonrasib, a small-molecule inhibitor made by California-based biotech Revolution Medicines, doubled the survival of patients with metastatic pancreatic ductal adenocarcinoma (mPDAC) compared to gold standard chemotherapy. While the median overall survival on chemo was only 6.6 months, those on the trial drug saw a median survival of 13.2 months.
A few more sips: Not being in this specific field myself, I immediately wanted to better grasp how this fits into the larger pancreatic cancer therapy picture. This gives context to the standing ovation.
It turns out that more than 90% of PDACs have a mutation in KRAS (part of the RAS family) that favors the ON state, driving lots of important cell pathways, including cell proliferation.
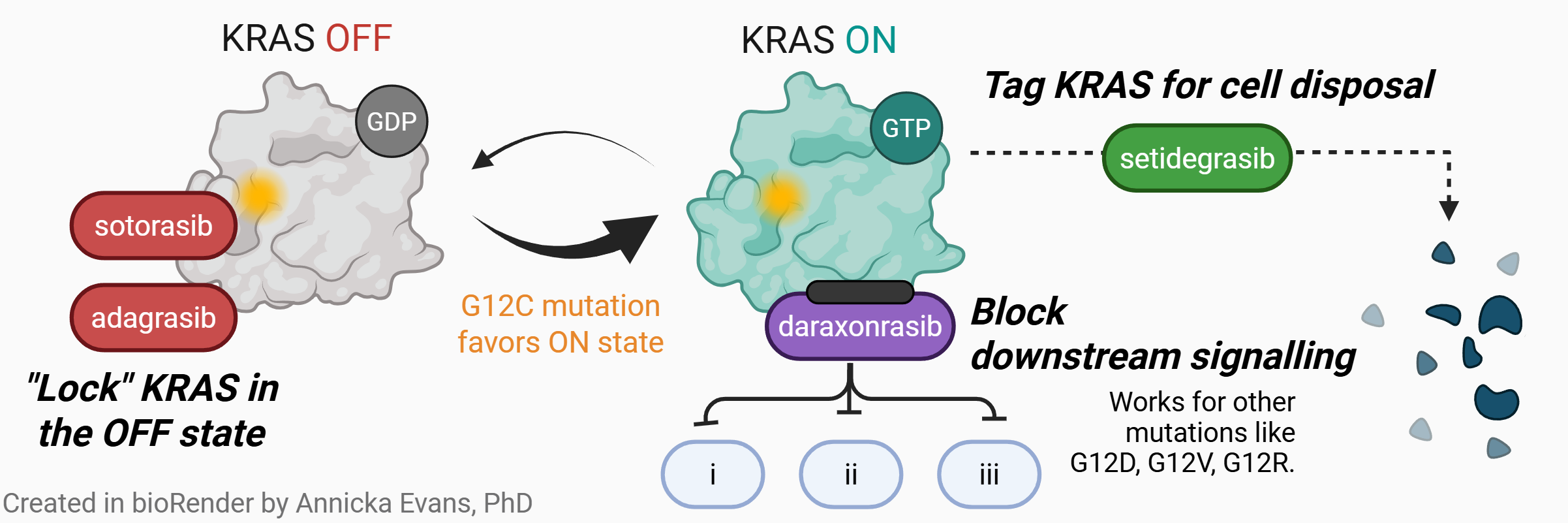
Small-molecule inhibitors that halt cell pathways, are not new, but it also turns out that KRAS has a particularly “smooth” binding domain and years of work in this space has yielded relatively few successes in blocking the pathway. Research in 2013 identified a “druggable” pocket which eventually led to the approval of two KRAS G12C (the particular mutation) inhibitors that try to lock KRAS in the OFF state — sotorasib and adagrasib. These two drugs, were celebrated upon their approval as well!
We also have a whole emerging modality called protein degraders that have been applied to the RAS pathway. The idea is to tag these proteins for the cell’s disposal machinery so they don’t even exist to propagate the cell proliferation pathways. In March, successful human data was reported on a degrader called setidegrasib, showing it could reduce tumors in lung and pancreatic cancer.
Finally, we get to daraxonrasib (which got the claps). Scientists at Revolution Medicines took the approach of blocking the binding site of RAS while in the ON state, preventing it from binding to proteins that are next steps in critical pathways (downstream signaling inhibition).
I hope this mini crash-course on KRAS and pancreatic cancer helps you understand the importance of the latest findings.
2. From the Bench
The Tea: While many gene therapies are targeting rare genetic diseases, Eli Lilly just released positive Phase 1 data for their gene editing drug, VERVE-102, in the heart disease space.
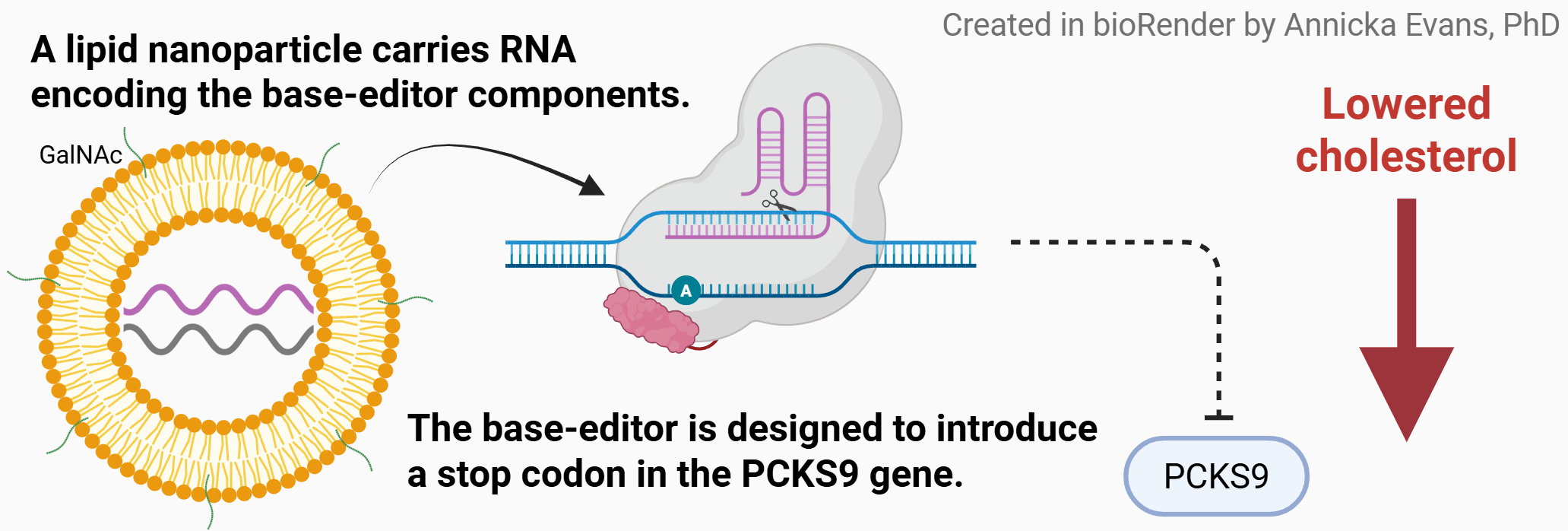
Besides not often hearing gene therapy and cardiovascular disease in the same sentence, what, in particular, is new about this? Well, we already know that inhibiting the PCSK9 gene in the liver results in reduced low-density lipoprotein (LDL) cholesterol, lowering risk of cardiovascular disease — currently, doctors can prescribe PCSK9 inhibitors in the form of an oral medication that needs to be consistently taken in order to see it’s long-term benefits to health.
VERVE-102 shifts the burden off the patient with a single IV dose that directly modifies the DNA in liver cells to perpetually turn-off (or lower expression of) the PCKS9 gene. The Phase 1b trial was tested in 35 individuals with hypercholesterolemia or premature coronary artery disease and in all but the lowest doses, there was a significant and lasting reduction in LDL.
A few more sips: I am not only looking forward to the future trial data on VERVE-102, but also VERVE-201, which uses the same platform technology but targets ANGPTL3 with the hopes of reducing both LDL cholesterol and triglyceride. That data isn’t expected until late next year or early 2028.
And while we’re talking about the line-up, I found it interesting that the earlier version of this drug (VERVE-101) showed liver toxicity and Lilly has said that their redesign of the lipid nanoparticle (LNP) carrier now minimizes that concern. The LNP now includes a particular sugar (GalNAc) that improves liver cell entry in a way that improves patient safety. VERVE-102 was already in their pipeline at the time of halting VERVE-101. An example of how an iterative pipeline can be beneficial.
Quick call back to issue No. 5 where we discussed another gene editor using LNPs (it was a split system with AAV carrying part too!) for the treatment of urea cycle disorders.
Message me if you have a recent science development you’d like to see featured!
3. Bio[Tech]
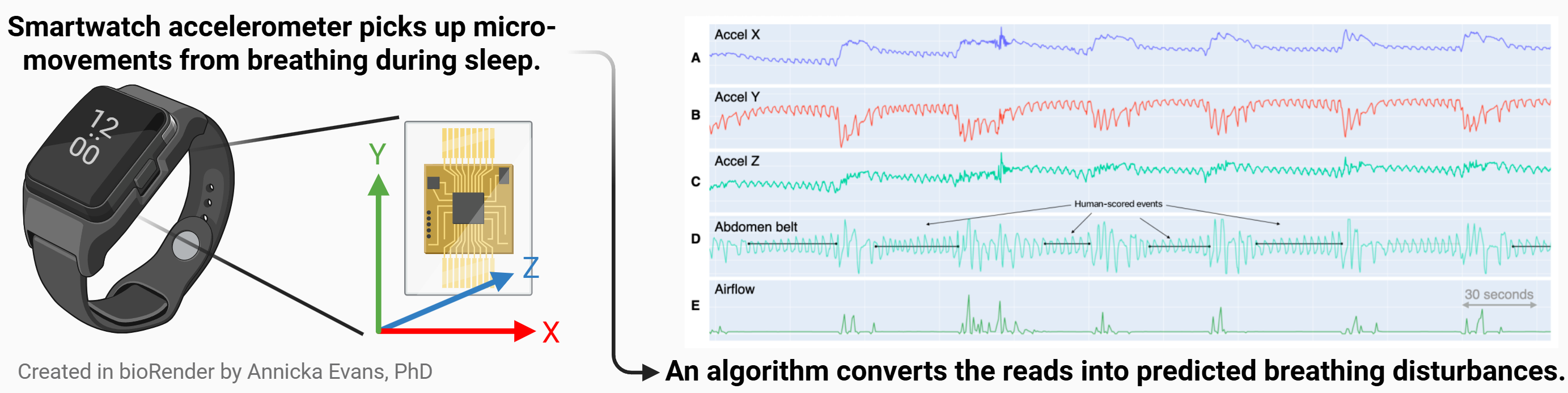
The Tea: Apple recently released a sleep apnea feature on the Apple watch, which evaluates disruptions in breathing during sleep.
Sleep apnea, which affects an estimated 30 million people in the U.S., is defined by what is known as apnea-hypopnea events or the apnea-hypopnea index (AHI). Apple has developed a new algorithm that takes motion readings from the watch’s triaxial accelerometer sensor and identifies what it thinks are breathing disturbances that could be apnea-hypopnea events. The consumer can review breathing disturbance values in application, but they will also be sent a notification if the algorithm detects an elevated disturbance read over a 30-day period, suggesting they may want to be evaluated for sleep apnea. Apple revealed data on their design, implementation, and validation phases, which included thousands of participants, in a white paper.
A few more sips: When it comes to wearables and wellness values, the major question is whether or not the proxy for a true diagnostic test will hinder (or unnecessarily prompt) proper care. To address this, Apple states in it’s technical white paper, that they took a cautious approach. While specificity for the alert was 98.5% (meaning you are very unlikely to get an alert if you do not have sleep apnea), sensitivity only came in at 66.5% (meaning the device will not alert quite a large portion of people who do have sleep apnea).
4. The Rulebook
The Tea: Late last week the U.S. Office of Management and Budget (OMB), which oversees the federal budget, released a proposal to significantly revise the way federal research grants are approved and what they can fund.
The proposed changes are open to public comment until July 13th.
Search for docket OMB-2026-0034 on www.regulations.gov to submit your comments. Include the section you’re commenting on in brackets (e.g. if the comment is for CFR 200.414, start your comment with [200.414]).
Some of the larger proposed changes? Agency senior appointees would be required to review all grants (and have ultimate veto power), the President’s policy priorities would be prioritized, grants could be terminated at any time, and the rules for what grant money can be used for gets much tighter (for example, needing pre-approval for conference attendance & not covering journal fees).
In part, the aim is to reduce spending, but they also state that the changes would keep activities “consistent with law and policy”, hold recipients “accountable when they fail to meet relevant standards”, and “ensure that basic American principles of equality and equal opportunity are upheld”.
A few more sips: I found this article by Elizabeth Ginexi incredibly helpful for breaking down the long list of proposed changes and what their implications are.

5. The Human Side
The Tea: Craig Spencer is an emergency medicine physician and public health professor at Brown University, but in this NYT piece he’s speaking as an Ebola survivor.
He contracted the virus during the outbreak of Zaire ebolavirus in West Africa between 2014 and 2016, which resulted in over 11,000 deaths and spread through 10 countries. Spencer carefully lays out why the current outbreak is so dangerous — from a geography riddled with violence, a species of ebolavirus with no vaccine or treatment, and a U.S. administration that has retreated from robust global humanitarian aid.

Biotech Term of the Week
Paid Subscriber Bonus Content
Grant Programs (FDA Encouraging Innovation series)
