
Organoids in space, split CRISPR, & the Narcissus of AI
No. 5 | April 9, 2026

📝 3-min survey: shape future issues & get a year of Biotech Term of the Week for $15 (available until April 20th)!
P.S. Already upgraded? I’ll add 6 months—just message me after the survey!
💬Lastly, I asked who was here in the chat and loved seeing the mix. Thanks for introducing yourselves and if you haven’t yet - go here!
Let’s get into this week’s cup of biotech tea. ☕ If you only have time for one this week, I’d start with #1!
An organ-on-a-chip was sent to space on Artemis II ➡️
A split-delivery AAV+LNP gene editing therapy ➡️
Conflicting trial results for a cardiac occlusion device ➡️
Updated Patient Preference Information guidelines ➡️
Is our use of AI akin to the Greek myth of Narcissus? ➡️
Bonus (paid): the make-or-break-it characteristics of a drug ➡️
1. Story I’m Watching
The Tea: The Artemis II mission to the moon (which had me absolutely entranced on Monday) has a biotech objective while traveling 250,000 miles away from Earth! Meet AVATAR (A Virtual Astronaut Tissue Analog Response), a thumb drive-sized organ-on-a-chip device used “to study the effects of increased radiation and microgravity on human health.” Each organ chip contains cells from the bone marrow of the Artemis II astronauts and they will be analyzed upon return to give insight into how space conditions affect people differently. There may also be information that can contribute to advancing personalized medicine on earth.

A few more sips: Bone marrow is extremely sensitive to radiation exposure and therefore very interesting to study in deep space. To make the chips, the astronauts donated platelets. Stem and progenitor cells were then purified out of the samples using magnetic beads that bind specifically to them. The cells were then loaded onto the chips with blood vessel cells and other supporting cells. NASA-funded scientists at Emulate, Inc. are behind the design of the organ-on-a-chip.
2. From the Bench
The Tea: Researchers at the Children’s Hospital of Philadelphia (CHOP) recently published a new split-delivery CRISPR approach for treating several urea cycle disorders (UCDs). In this system, lipid nanoparticles (LNPs) deliver the genetic instructions to produce the editing machinery, while adeno-associated virus (AAV) delivers the guide RNA that directs where the editing should occur. This split-delivery strategy allows for longer and more complex guide RNA packages that are difficult to chemically synthesize but important for making needed edits for certain UCDs.
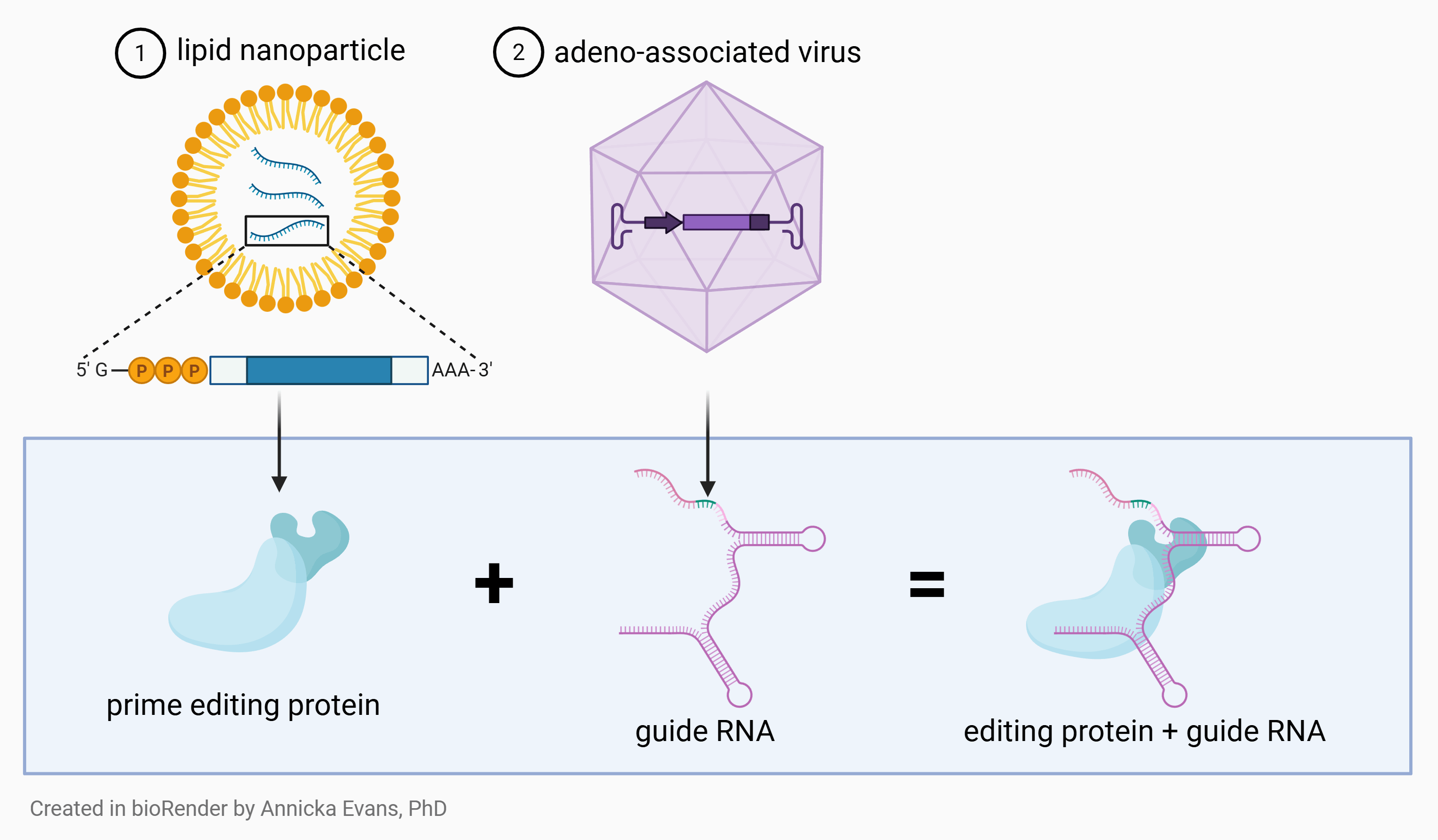
The AAV + LNP therapy uses prime editing as opposed to base editing - two slightly different versions of CRISPR technology. While base editing is limited to making single-letter DNA changes, prime editing can make a broader range of changes, expanding the types of diseases that may be treatable.
A few more sips: You may have seen the story last year of Baby KJ receiving a world’s first personalized CRISPR gene therapy for his rare genetic liver disease. Dr. Rebecca C. Ahrens-Nicklas at CHOP led both that work and this latest proposal to the FDA. Earlier this year, the team published both the science and the pre-IND feedback they received for AAV + LNP approach.
If you’re interested in the FDA’s pre-IND feedback, you can read it here.

Message me if you have a recent science development you’d like to see featured!
3. Bio[Tech]
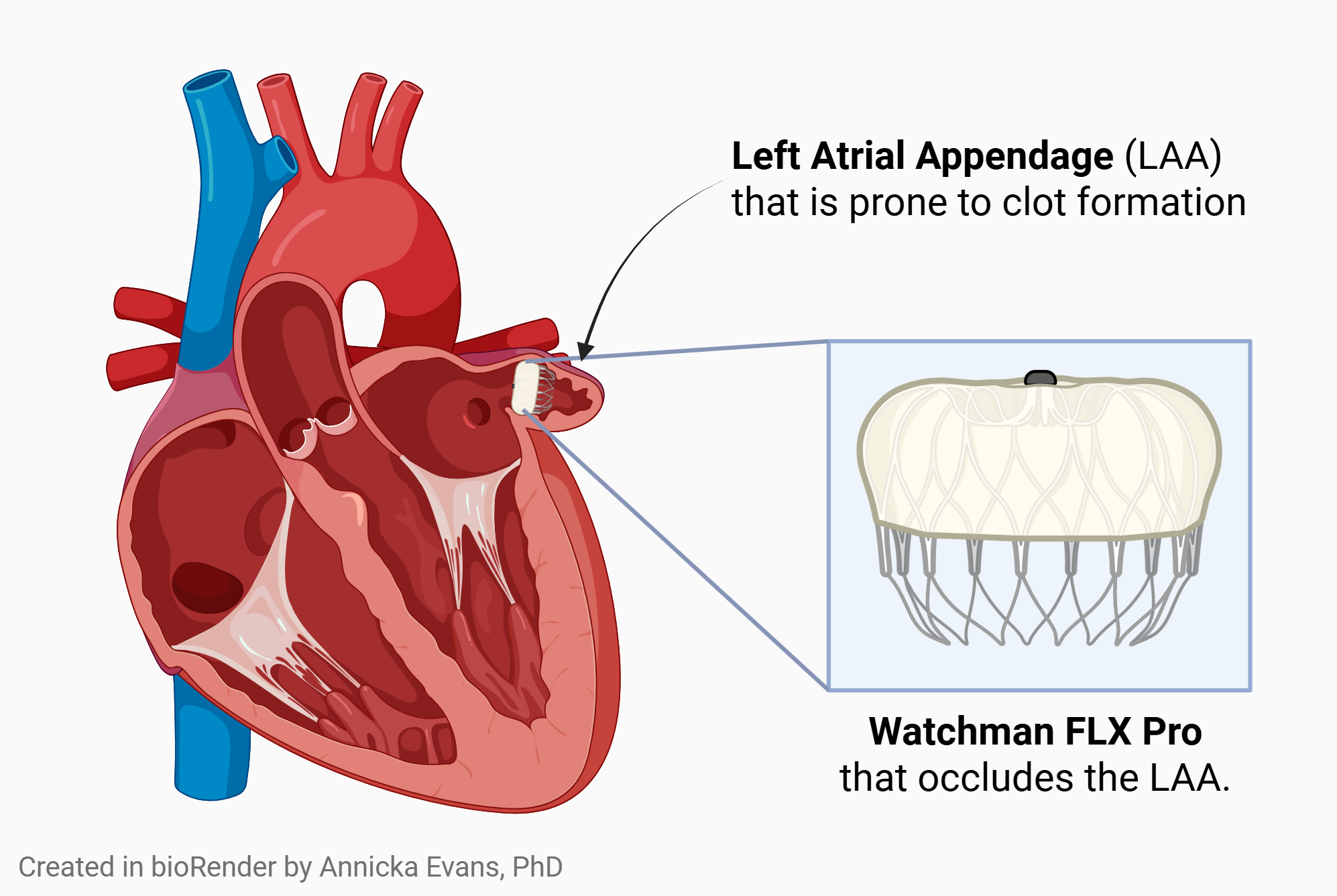
The Tea: Two recent trials reached different conclusions about whether a left atrial appendage (LAA) occlusion device can safely replace non-vitamin K oral anticoagulants to reduce stroke risk in patients with atrial fibrillation. Devices like the Watchman FLX Pro (Boston Scientific) are currently approved in patients who can’t take anticoagulants, but not yet as an alternative for those who can. The larger trial found the device was noninferior (think similar) to anticoagulation therapy. The smaller trial found it was NOT noninferior (think not similar). Why the uncertainty? The total number of stroke events across both studies was low, leading to wide confidence intervals and less precise conclusions.
Quick call back to last week when we talked about the Lyme vaccine trial narrowly missing its endpoint because of low Lyme disease events!
A few more sips: The CHAMPION-AF trial was the one that concluded the device may be similarly safe to anticoagulation. While it was a larger trial (3000 enrolled), critics note that it was sponsored by Boston Scientific and they only used their Watchman FLX Pro device. We also see that the baseline risk of stroke in the patient population averaged somewhat low, potentially making the device appear more favorable.
Conversely, the CLOSURE-AF trial concluded anticoagulation is likely still the safest treatment. This study was not industry funded, used 2 different occlusion devices (Boston Scientific Watchman FLX Pro and Abbott Amplatzer), but only enrolled 900 patients. It’s population baseline risk of stroke averaged higher, also potentially impacting results.
Read this editorial piece for a deeper review on what to make of these conflicting results.
My first question was: why implant a device at all if anticoagulants already work? The authors note that expanding the indication allows physicians and patients another option to explore through shared clinical decision-making. It was also noted that many patients do not consistently take blood thinners, reducing their effectiveness.
4. The Rulebook
The Tea: This week the FDA released updated guidance on how patient input can be collected and used in medical device approval decisions which are regulated by the Center for Devices and Radiological Health (CDRH). This input - called Patient Preference Information (PPI) - captures how patients weigh benefits and risks of medical devices. While PPI has never been required, the FDA continues to emphasize its value in decision-making.
The biggest shift in this update? In 2016, PPI was primarily considered in select novel or higher-risk approval pathways (PMA, HDE, or De Novo). Now, the FDA is explicitly extending its use across the entire life cycle, including 510(k) submissions and even postmarket decisions.
As a quick frame of reference, the patient voice framework for drugs and biologics is called Patient-Focused Drug Development (PFDD).
A few more sips: An important reminder (that I needed to give myself when reviewing this): PPI is not used to approve something that’s unsafe. It’s used when risks are acceptable and patient opinion can help interpret risk/benefit analysis. It sits in the gray area between regulatory protection and patient autonomy. Here’s an example from the guidance showing how PPI may be used to inform a device decision:
A permanent, fully implantable hearing device under review shows higher risk of facial nerve injury than similar devices already on the market. PPI revealed that a sizeable group of patients highly valued the discreet design of the device and would be willing to accept the increased risk. In this example, the FDA may use that patient preference information to determine that the device’s benefits outweigh the risks for the intended population.
A great in-depth article by The FDA Group for those interested:

5. The Human Side
The Tea: In this opinion piece by Ezra Klein entitled ‘“I Saw Something New in San Francisco”, Ezra Klein walks us through a striking analogy between our collective obsession with AI and the Greek myth of Narcissus. He reminded me that the story doesn’t convey an obsession with self but with an extension of self in any material other than self. And what is AI if not that? We regularly warn each other of the selection bias that comes from using LLMs and that the way we frame our prompts creates a self-reinforcing loop akin to staring at our own reflection. A thought-provoking read as we continue into this new era.
A few more sips: Beyond the analogy, Klein describes how he sees us giving AI more and more access to both our work and our personal lives. It’s a double-edged sword. The more information AI has about something, the better it’s responses become. But he points out that the nature of that information might change if we know it has an audience.
“I know people who have been keeping a journal for years and now upload it into any new A.I. system they use. The journal has become, for them, not just a place to pour out their innermost thoughts, but a convenient package of context that can be used to make themselves known to new systems, and thus make the systems more useful to them. But that of course changes how they write in those journals: What was once private now has a reader.” - Ezra Klein
Biotech Term of the Week
Paid Subscriber Bonus Content (this is the last week it will be free to preview!)
Reminder: The Biotech Term of the Week is where I break down one concept you’ll encounter again and again in biotech. Seeing it here makes it become clearer, more intuitive, and easier for you to speak about with confidence.
Critical Quality Attribute (CQA)
non biotech synonym: make-or-break characteristic
While a product or drug can have dozens of qualities that are measured, a critical one is something that could directly impact patient safety or how well it works.
Officially, CQAs are defined in ICH Q8 as “physical, chemical, biological, or microbiological properties or characteristics that should be within an appropriate limit, range, or distribution to ensure the desired product quality.”
These attributes are:
continuously monitored throughout development, and
given acceptable upper and lower bounds based on what is known (or predicted) not to impact safety or efficacy.
It’s important that they are defined early on in drug development so that you can carefully monitor any changes. This helps guide process understanding and risk-based decision-making.
Here are some examples of how process steps are tied to CQAs and why it’s important to control them early:
Does your ultra-filtration step reduce your concentration?
Concentration is a CQA, so you’d want to control or adjust this step.
Does your antibody lose binding affinity after storage?
Binding is a CQA, so you’d need to carefully evaluate stability temperatures and times.
Does a purification step fail to remove impurities?
Certain residuals are CQAs, so that step may need to be replaced or another purification step added.
Does a candidate cell line lead to a less ideal glycosylation pattern?
Post-translational modification may be a CQA, so a different cell line may need to be selected.
As you can see, once a CQA is defined, any part of the process that impacts it is carefully studied and tightly controlled. This leads directly into another term for a future week… a critical process parameter (CPP)!
